What is a cleft palate?
The palate is the roof of the mouth and also forms the floor of the nose. It has two parts: the hard palate in the front, which is made of bone, and the soft palate in the back, which is made of muscle.
A cleft is a gap, separation, or opening that results from abnormal fetal development. A cleft palate is a birth defect that occurs when the tissues of the palate do not fuse properly during early fetal development, typically between the 8th and 12th weeks of gestation.
Cleft palate can range in severity. It may involve only the muscles of the soft palate (called a submucous cleft palate, Fig. 1), or it may include a complete separation of the bone and tissue of both the hard and soft palate (Fig. 2). In some cases, a cleft affects only the soft palate (Fig. 3). A cleft of the hard palate always includes a cleft of the soft palate.
Surgery is required to repair a cleft palate.

Fig. 1 – Submucous cleft palate

Fig. 2 – Cleft of hard and soft palate

Fig. 3 – Cleft of soft palate
What causes a cleft palate?
Despite years of research we still do not have a great understanding of why cleft palates occur. Most doctors and scientists agree that clefts are a combination of genetic as well as environmental factors including drugs, infections, maternal illness, and possibly vitamin deficiencies.
Some children with cleft palate may also have other congenital differences. These can range from easily recognized conditions to ones that are more difficult to detect. However, most children born with a cleft lip and/or palate are otherwise typically developing, healthy children.
How do I feed my child with a cleft palate?
Feeding may be different for babies born with a cleft palate. Because there is an opening in the roof of the mouth, many babies are not able to create the suction needed for breastfeeding or for using a standard bottle. That can make feeding more challenging and it’s completely normal to need extra support.
Every baby’s needs are different, so it is important to talk with your doctor or feeding specialist about the best feeding approach for your child. If you are having difficulty feeding your baby or have questions about feeding at home, please call our office. Our care team can provide guidance and support.
Why is a cleft palate repaired?
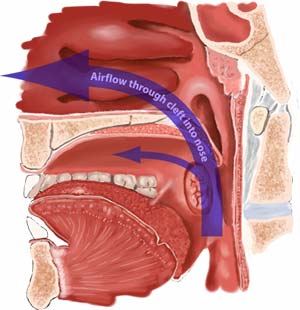
Fig. 4 Nasal air escape
If a child can eat and drink with a cleft palate, you may wonder why a cleft palate needs to be repaired at all. The reason is simple—speech. Most human speech and language requires regulation of air flow through the nose and mouth. If air leaks out of the nose while we are speaking, many of the sounds we make do not sound right. When a lot of air leaks out of the nose, our speech becomes almost unintelligible.
A child with an unrepaired cleft palate cannot stop air from escaping the nose during speech (Fig. 4). This makes it very difficult for a child to learn how to speak correctly. It also makes it difficult for others to understand their speech.
How is a cleft palate repaired?
The repair of a cleft palate requires reconstructive surgery and general anesthesia. The cleft is repaired by bringing the tissues around the cleft together (Fig. 5).

Fig. 5 – Cleft palate before and after repair.
When is the right time for cleft palate surgery?
Cleft palates are typically repaired between 10 and 12 months of age. Many variables must be considered to determine the best time to repair a cleft palate. Depending upon the size of the cleft palate the surgeon may require that the baby wean from the bottle prior to palate repair.
In addition, the baby’s birth history, gestational age, general health, growth and development, parent preference and family leave, as well as other individual factors, may influence timing for cleft palate repair surgery.
Submucous cleft palates are not necessarily repaired early in life. A submucous cleft only needs to be repaired if speech and language are affected. Approximately 50% of children with a submucous cleft palate will require surgery to repair it. It is usually possible to determine the need for submucous cleft palate repair between 3 and 6 years of age.
Are there any instructions I need to follow before cleft palate surgery?
Your child must have a physical examination by their pediatrician or family doctor within 7 days before surgery to make sure they are in good health. The doctor you see needs to complete the History and Physical form provided by our office. You must bring the completed form with you the day of surgery.
For your child’s safety, it is very important that they have an empty stomach when anesthesia is given. Please follow our preoperative eating and drinking guidelines. If you do not follow these guidelines, your child’s surgery will be cancelled.
What can I expect after surgery?
Cleft palate repair surgery usually takes between 2 and 3 hours. Your doctor will speak with you as soon as the surgery is complete.
After surgery, your child will wake up in the recovery room, which may take 45 minutes to an hour. Once awake, your child will be admitted to the hospital. You may accompany your child when they are transferred to your hospital room. One or both parents may stay with their child throughout the hospital stay, and we encourage at least one parent to remain with their child during hospitalization.
Following surgery, your child will have soft arm splints in place. These splints help prevent hands or objects from being placed in the mouth while the palate heals. The splints may be removed while you are holding your child and can closely supervise them. At all other times, the arm splints should be worn for two weeks after surgery.
Children typically begin drinking by mouth 24 to 36 hours after surgery. Until then, fluids are given through an intravenous (IV) catheter. Most children are discharged from the hospital after two nights. In some cases, a child may need a longer hospital stay if there are feeding concerns or additional time is needed for pain control.
How should I take care of my child after surgery?
No special wound care is needed after cleft palate surgery.
After you are discharged from the hospital, you may give acetaminophen (Tylenol®) or ibuprofen (Children’s Motrin®) for pain control. During the first two weeks after surgery, you may notice white areas along the inside borders of the teeth when looking at the roof of your child’s mouth. These areas are normal scabs that form as the palate heals. They are not a sign of infection and will gradually disappear.
Your child will need to follow a puréed diet for two weeks after palate repair. Foods such as vegetable purées, yogurt, and applesauce are appropriate. In some cases, children may need to transition off the bottle before surgery so they can drink from a cup during recovery.
After two weeks, your child may return to their regular diet. Many families choose to keep their child home from daycare for about two weeks following cleft palate surgery.
Follow‑up visits and healing after surgery
A postoperative follow‑up visit is usually scheduled 4 to 8 weeks after surgery. During this visit, your doctor will examine the palate to assess healing and ensure recovery is progressing as expected.
Dissolving stitches are used to repair the palate. These stitches gradually dissolve over 4 to 6 weeks. It is common to see stitches along the center of the palate for several weeks after surgery, including up to a month.
Where to find cleft palate surgery treatment?
Cleft palate surgery is provided by our ENT and facial plastic surgery team at Children’s Minnesota. Care is available at our Minneapolis and St. Paul campuses.
To schedule a consultation, please call: 612-874-1292.
Questions?
This information is not specific to your child and provides general information. If you have any questions, please call your nearest Children’s Minensota ENT and facial plastic surgery clinic.

