Spina Bifida + MWFCC
In 2016, our center performed our first fetal repair of myelomeningocele (MMC), the most severe form of spina bifida. Led by a team of medical experts in the field of fetal diagnosis and therapy, our program has grown to become a high volume MMC fetal surgery center. As of Dec. 3, 2025, the Midwest Fetal Care Center has evaluated more than 193 women for maternal-fetal surgery for spina bifida; 124 have chosen to undergo surgery.
Maternal characteristics of fetal MMC repair patients
30.7 years
Average maternal age at surgery
25.0 weeks
Average gestational age at surgery
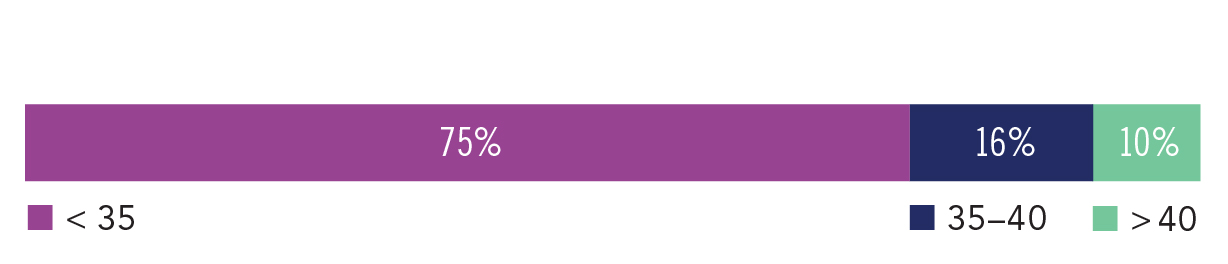
Maternal BMI category (kg/m2)
Maternal outcomes after fetal MMC repair*
| Outcome Metric | Open | Fetoscopic | MOMS Trial |
|---|---|---|---|
| Maternal survival | 57 of 57 (100%) | 45 of 45 (100%) | 78 of 78 (100%) |
| Membrane separation* | 13 of 57 (23%) | 23 of 45 (52%) | 20 of 78 (26%) |
| Abruption+ | 1 of 57 (2%) | 0 of 45 (0%) | 5 of 78 (6%) |
| Maternal transfusion at delivery | 0 of 57 (0%) | 0 of 45 (0%) | 7 of 78 (9%) |
| Dehiscence of hysterotomy at delivery | 0 of 57 (0%) | 0 of 45 (0%) | 8 of 76 (11%) |
Data for 2/1/2016–7/31/2024 | Format: average ± standard deviation
*Indicates any membrane separation (the most sensitive definition); this is potentiality different than the definition applied in the MOMS trial.
+ Placental abruption within 7 days of fetal surgeryCandidates evaluated for fetal MMC repair
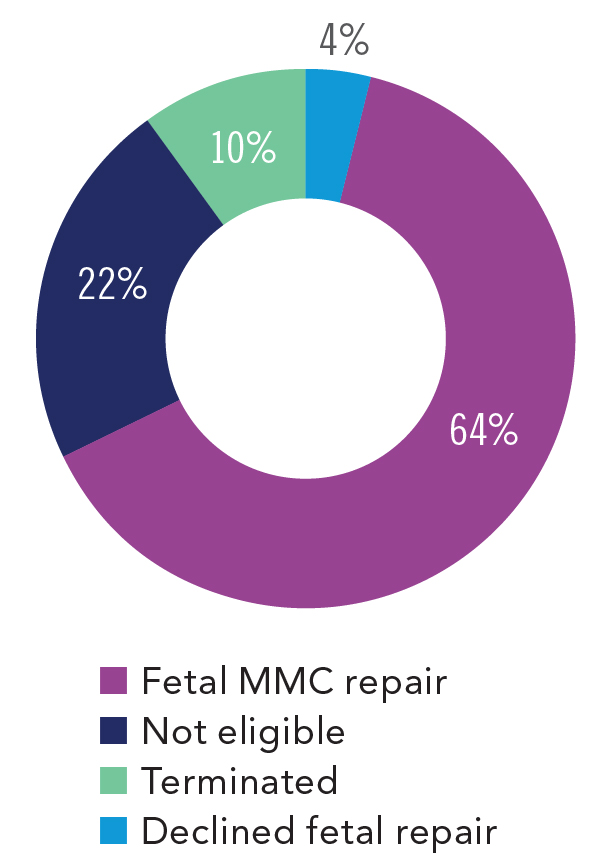
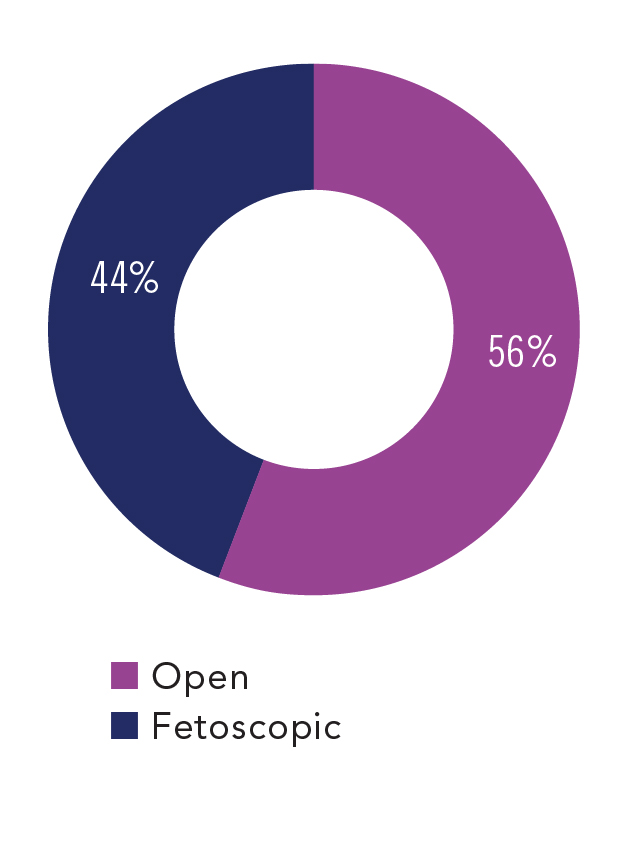
Fetal repair surgical method
The MOMS and MOMS2 trials
The Management of Myelomeningocele Study (MOMS Trial) was a 7-year, multi-center, randomized clinical research trial that comprehensively studied the outcomes of open fetal surgery for repair of spina bifida compared to a traditional postnatal repair.1 The MOMS Trial included 183 surgically eligible patients, who were randomized to either fetal or postnatal MMC repair. Of those analyzed, 80 patients underwent post-birth surgical repair and 78 underwent open fetal surgery for spina bifida. Overall, the MOMS Trial concluded that prenatal surgery for myelomeningocele reduced the need for hydrocephalus-related neurosurgical interventions at 12 months, including cerebrospinal shunt placement, and improved motor outcomes at 30 months versus postnatal repair, but was also associated with maternal and fetal risks. The MOMS Trial is seen as the industry benchmark for this treatment, and here we describe how our outcomes compare to those from this seminal study.
In addition, to study the long-term impact of maternal-fetal surgical closure of spina bifida versus post-natal management, more than 150 patients from the original MOMS trial were enrolled into follow-up studies to a compare childhood outcomes (MOMS2). In a secondary analysis, 51.3% of children who underwent prenatal repair could independently walk community distances compared with 23.1% of children who underwent standard postnatal repair.2 Additional long-term benefits of prenatal surgery included improved independent functioning as well as fewer surgeries for shunt placement and revision.3, 4 In addition, overall urodynamic findings were improved with the prenatal versus post-natal repair groups with fewer infants requiring intermittent catheterization and more infants voiding on their own with prenatal surgery.5 Finally, parents of children repaired prenatally report significantly higher quality of life scores and lower mean family impact scores when compared to postnatally repaired patients.4 Overall, these secondary analyses found that the benefits of prenatal repair reported at age 30 months persisted into school age.
Open vs. fetoscopic maternal-fetal surgery
For patients who are eligible for maternal-fetal surgery for spina bifida, the center offers two different surgical access strategies, open and fetoscopic. Open maternal-fetal surgery for spina bifida requires a maternal surgery technique known as a hysterotomy, which is the making of an approximately 6 cm incision in the uterus, to access the unborn baby. After an open maternal-fetal surgery, the baby and all future pregnancies have increased risk and must be delivered by cesarean section.6
For certain patients, a minimally invasive fetoscopic approach is offered at our center to reduce the risks associated with a hysterotomy and allow for the potential of a vaginal birth. In a fetoscopic repair, the surgery is completed through three 5-mm incisions in the uterus using a small camera, known as a fetoscope, and laparoscopic instruments. The fetal repair technique is the same for both the open and fetoscopic surgical access methods.
We discuss all available medical options including open vs. fetoscopic prenatal surgery or post-birth management with our patients to create a care plan that works best for each individual family.
Here we present outcomes for both our open and fetoscopic surgeries compared to the open surgery outcomes reported by the MOMS trial.
Outcomes after fetal MMC repair
55%
showed improved motor function
| Outcome Metric | Open | Fetoscopic | MOMS Trial |
|---|---|---|---|
| Surgical mgmt of hydrocephalus, 12 mo* | 16 of 51 (31%) | 15 of 33 (46%) | 31 of 78 (40%) |
| Difference between motor function and anatomical levels† | Age at pediatric function assessment | neonatal | neonatal | 30 months |
| ≥ Two levels better | 23 of 54 (43%) | 16 of 37 (43%) | 20 of 62 (32%) |
| One level better | 13 of 54 (23%) | 9 of37 (24%) | 7 of 62 (11%) |
| No difference | 3 of 54 (6%) | 4 of 37 (11%) | 14 of 62 (23%) |
| One level worse | 9 of 54 (17%) | 7 of 37 (19%) | 13 of 62 (21%) |
| ≥ Two levels worse | 6 of 54 (11%) | 1 of 37 (3%) | 8 of 62 (13%) |
Data for 2/1/2016–1/25/2023
*Surgical management included shunt (n=7 open, 3 fetoscopic) or ETV (n=6 open, n=1 fetoscopic)
†For the difference between the neonatal motor function level and the anatomical level (pre-birth ultrasound), “better” indicates function that is better than expected on the basis of the anatomical level. Of note, these are preliminary results based on lower-level extremity movement in the NICU. Results may change as children develop due to better ascertainment.
Maternal outcomes and delivery
Since July 31, 2024, 57 mothers have elected to undergo open fetal repair of MMC and 45 mothers have elected to undergo fetoscopic fetal repair at our center. The average post-surgery length of stay was three days for the last 15 patients. Mothers are typically discharged home and further post-surgery care is co-managed with the mother’s referring maternal-fetal medicine specialist. For the open fetal repair patients, cesarean section deliveries are scheduled for approximately 36 weeks gestation at our center, while fetoscopic repair patients may carry until the onset of labor, or until delivery is otherwise medically indicated.
Of the fetoscopic closures that survived until delivery, 19 of 43 (44%) gave birth vaginally. Thirteen of the 19 (68%) of vaginally delivered mothers carried longer than 36 weeks.
The majority of patients spent less than a week in the hospital before delivery, and around three days in the hospital after delivery. Our team makes every effort to minimize any potential maternal complications related to the fetal repair.
Outcomes after fetal MMC repair
Due to transfers of care back to local providers for delivery and follow-up, pediatric outcome data is currently available for only a small subset of our patients. Efforts are underway to connect with external patients to gather more complete pediatric outcomes data.
Hydrocephalus, or brain swelling, can occur in babies with spina bifida and is typically treated by diverting cerebrospinal fluid using a surgical procedure (endoscopic third ventriculostomy, ETV) or by permanently placed brain shunt.
The MOMS Trial showed important benefits to infants that underwent fetal repairs, including a reduction in the need for shunt/ETV from 82% (postnatal repair) to 40% during the first 12 months of life.1 Overall, the patient data from our center is similar to the outcomes reported in the MOMS Trial, with a 34% rate of surgical management of hydrocephalus.
In addition, 67% of our fetal fMMC repair patients showed an improvement in motor function in the neonatal period compared to the function predicted by their prenatal imaging (prior to MMC repair).
These results are preliminary and may change as children develop due to better ascertainment; however, these findings are consistent with the MOMS trial, and the impact of the prenatal repair was also seen into childhood (MOMS2).1, 4
Urinary, bladder and bowel dysfunction may occur in babies with spina bifida due to the nerve damage caused be the spine defect. A MOMS Trial companion paper found that at 30 months, the fetal MMC repair group had a clean intermittent catheterization (CIC) rate of 38%.5 Long-term, the MOMS2 childhood data showed CIC rates of 62% vs 87% for the prenatal and postnatal groups respectively defined as requiring catheterization three or more times per day.7 The data currently available for our center shows a 9% CIC rate at 12 months (5/54 patients). Reoccurring urinary tract infections (UTIs) occurred in 2% (1/54) of our fetal repair patients, and constipation in 50% (27/54). Our center is in the process of collecting our bladder and bowel outcomes for future reporting.
Neonatal outcomes after fetal MMC repair
| Outcome Metric | Open | Fetoscopic | MOMS Trial |
|---|---|---|---|
| Neonatal survival to delivery | 57 of 57 (100%) | 43* of 45 (96%) | 77 of 78 (99%) |
| Neonatal survival post-delivery | 56 of 57 (98%) | 43 of 43 (100%) | 76 of 77 (99%) |
| Average GA at delivery (weeks) | 34.5 ± 2.6 | 35.0 ± 3.7 | 34.1 ± 3.1 |
| Average Birthweight, g | 2390 ± 612 | 2478 ± 683 | 2383 ± 688 |
| Apnea† | 17 of 53‡ (32%) | 10 of 37 (27%) | 28 of 77 (36%) |
Data for 2/1/2016–7/31/2024 | Format: average ± standard deviation
*One spontaneous intrauterine fetal demise (IUFD) occurred at 29 weeks with no identifiable cause, one at 33 weeks due to cord entanglement with >30% membrane separation.
†Definition: true cessation of breathing during rest that results in the need for caffeine due to apnea-based symptoms (not given prophylactically) or home-monitor at NICU discharge.
Neonatal outcomes after fetal MMC repair
37%
required surgical intervention
2 Houtrow AJ, MacPherson C, Jackson-Coty J, et al. Prenatal repair and physical functioning among children with myelomeningocele: a secondary analysis of a randomized clinical trial. JAMA Pediatrics. 2021;175:e205674-e205674.
3 Farmer DL, Thom EA, Brock JW 3rd, et al. Management of Myelomeningocele Study Investigators. The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes. Am J Obstet Gynecol. 2018; 218:256.e1-256.e13.
4 Houtrow AJ, Thom EA, Fletcher JM, et al. Prenatal repair of myelomeningocele and school-age functional outcomes. Pediatrics. 2020;145:e20191544.
5 Brock JW III, Carr MC, Adzick NS, et al. Bladder function after fetal surgery for myelomeningocele. Pediatrics. 2015;136:e906–13.
6 Goodnight WH, Bahtiyar O, Bennett KA, et al. Subsequent pregnancy outcomes after open maternal-fetal surgery for myelomeningocele. American Journal of Obstetrics and Gynecology. 2019;220:494.e1-494.e7.
7 Brock III JW, Thomas JC, Baskin LS, et al. Effect of prenatal repair of myelomeningocele on urological outcomes at school age. The Journal of Urology. 2019;202:812-818.
Our goal is to provide our patients and community the latest patient outcomes data to support informed decision making. We encourage you to reach out to other health care systems to request and review their outcomes data in order to utilize the information available when evaluating your health care options.
See our other outcomes
