What is congenital diaphragmatic hernia (CDH) and where to find congenital diaphragmatic hernia treatment?
The diaphragm muscle divides your chest and abdomen and it helps with breathing.
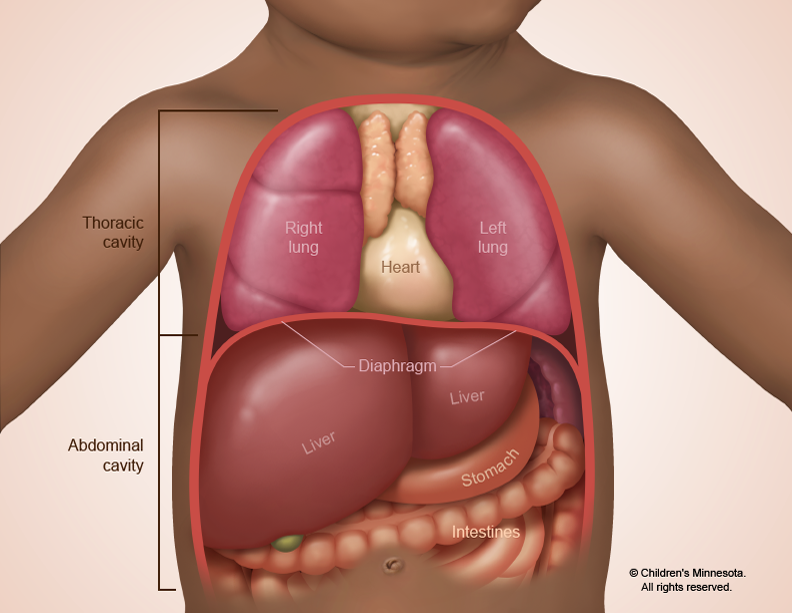
It is a serious condition because the organs press against the baby’s lungs and interfere with their normal growth. Congenital diaphragmatic hernia is thought to occur in about one in 2,500 babies. Congenital diaphragmatic hernia treatment is available at Midwest Fetal Care Center.
Who will be on my care team?
At Midwest Fetal Care Center, a collaboration between Children’s Minnesota and Allina Health, we specialize in individual attention that starts with you having your own personal care coordinator to help you navigate this complex process. We use a comprehensive team approach for congenital diaphragmatic hernia treatment. That way, you are assured of getting the best possible information by some of the most experienced physicians in the country. Your care team will include a maternal-fetal specialist, a pediatric surgeon, a neonatologist, a fetal cardiologist, a geneticist, a nurse specialist care coordinator, a fetal care clinical social worker, and several other technical specialists. This entire team will follow you and your baby closely through the evaluation process and this team will be responsible for designing and carrying out your complete care plan.
What causes congenital diaphragmatic hernia?
Like most birth defects, it’s unknown what causes congenital diaphragmatic hernia. There are rare familial cases where a parent or a relative may be affected, but in most cases, we don’t know what causes CDH.
How is congenital diaphragmatic hernia diagnosed?
Congenital diaphragmatic hernia can be detected by ultrasound as early as 16 weeks in pregnancy. When abdominal organs such as the intestines or stomach are seen in the chest cavity of the developing fetus, CDH is strongly suspected. Unfortunately, we still see many patients each year who receive a congenital diaphragmatic hernia diagnosis after birth. When this occurs, the newborn may be severely ill before doctors or other caregivers realize the problem.
How is congenital diaphragmatic hernia managed before birth?
The prenatal management of babies with congenital diaphragmatic hernia starts with acquiring as much information about the CDH as possible. To that end, we will use several different techniques such as high resolution ultrasound, fetal echocardiography and MRI to gather this information.
What is high-resolution fetal ultrasonography?
High resolution fetal ultrasonography (US) is a non-invasive test performed by one of our ultrasound specialists. The test involves looking at your baby through the mother’s abdomen using an ultrasound probe. If we see abdominal structures at the same level as the heart on US, the presence of a diaphragmatic hernia is confirmed. In some cases, US can visualize the hole in the diaphragm, making the diagnosis very clear.
The presence of liver in the thoracic cavity generally predicts a worse outcome for congenital diaphragmatic hernia. Therefore, position of the fetal liver is also assessed during fetal US.
What is the lung-to-head ratio and how is it used for babies with congenital diaphragmatic hernia?
The lung-to-head ratio (LHR) is an important measurement that helps us to predict how severe your baby’s CDH may be. It is obtained by measuring lung area at the level of heart and dividing by the head circumference. A low LHR (less than 1.0) is associated with more severe disease.
What is a fetal echocardiogram?
Fetal echocardiography (“echo” for short) is performed at our center by a physician who specializes in fetal heart abnormalities. This is a non invasive high resolution fetal ultrasound that involves looking specifically at your baby’s heart through the mother’s abdomen using an ultrasound probe. This test is important because about one of every ten patients with congenital diaphragmatic hernia can also have a serious heart abnormality.
What is a fetal MRI?
MRI stands for magnetic resonance imaging. It is another non-invasive test we use to find out as much information as possible about your baby’s CDH. This test involves the mom and baby being scanned while partially inside our MRI machine. The test is a bit loud, but only takes a few minutes and is not uncomfortable.
What happens after my evaluation is complete?
After we have gathered all of the anatomic and diagnostic information, our full team will meet to discuss the results of your testing and then share our recommendations and options for congenital diaphragmatic hernia treatment with you. Our approach for fetuses with CDH is twofold. First, we monitor the mother and the baby very carefully during pregnancy looking for any potential complications, such as premature labor or excessive amounts of amniotic fluid that might lead to premature delivery. Second, we try to predict the severity of CDH based on ultrasound and MRI findings so we can be prepared during and after delivery to optimally care for your infant.
How is congenital diaphragmatic hernia treated after birth?
Our goal for every patient is to have your baby get as close to your due date as possible. Most babies with congenital diaphragmatic hernia are born vaginally near term. Your baby will be born at The Mother Baby Center at Children’s Minnesota and Abbott Northwestern. Children’s Minnesota is one of only a few centers nationwide with the birth center located within the hospital complex. This means that your baby will be born just a few feet down the hall from our newborn intensive care unit (NICU). Additionally, many of the physicians you have already met will be present during or immediately after your baby’s birth so we can care for your baby right away.
Because congenital diaphragmatic hernia interferes with normal lung development, our immediate concern at birth is to ensure that your baby has good breathing. This may require using a mechanical ventilator. A ventilator requires inserting a tube into the baby’s windpipe that is connected to a ventilator machine. We also may administer medications that improve blood flow through the lungs and help blood vessels in the lungs to relax. In addition, we use artificial or intravenous nutrition to help the baby remain nourished until we’re able to use the mother’s breast milk.
What is ECMO?
ECMO is an acronym for extracorporeal membrane oxygenation. This is an advanced technology that’s used in cardiac bypass surgery and is available at only a very few specialized centers nationally. For CDH, ECMO is used in those babies who have the most severe form, roughly one third of all fetuses with this diagnosis. If standard therapy, such as a ventilator or medication, is not working, the next treatment is ECMO. ECMO does the work of the baby’s heart and lungs until they can recover. At Children’s Minnesota, we have one of the nation’s best outcomes for patients requiring ECMO.
When will my baby have the congenital diaphragmatic hernia operation?
The hole in the diaphragm will need to be surgically repaired.
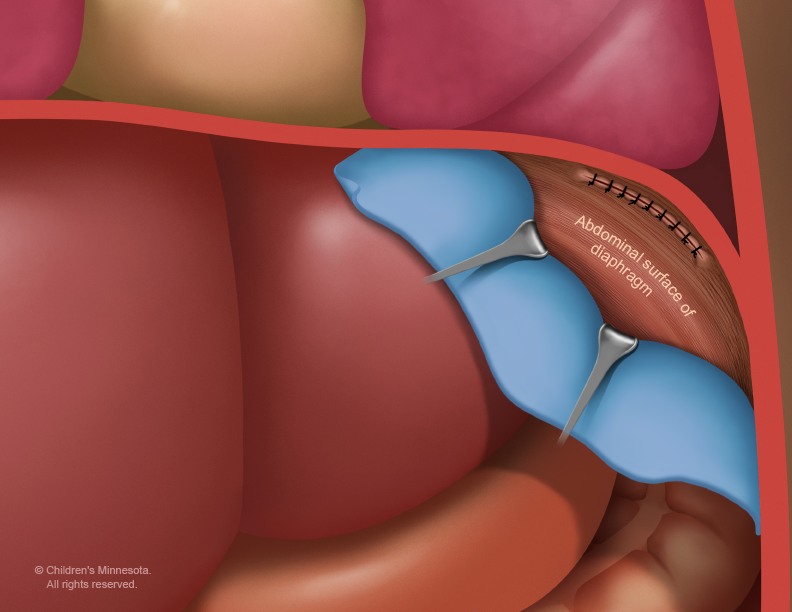
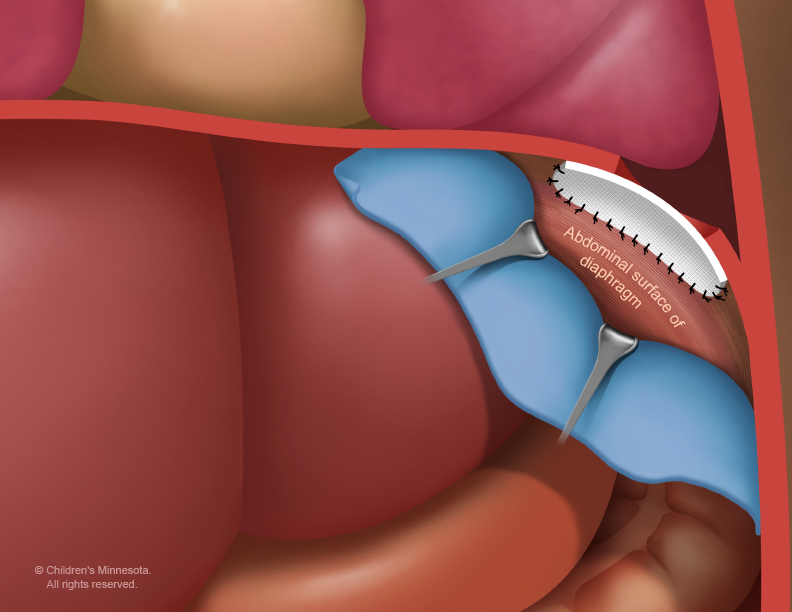
However, this surgery is not an emergency and frequently it is delayed for several days or weeks until we are certain that your baby is in the best possible condition for surgery.
What is my baby’s prognosis?
There is a wide range of outcomes and prognosis for children with congenital diaphragmatic hernia. Nationally, babies with severe disease requiring ECMO only have about 50% survival, while babies with CDH that do not require ECMO have about 90% survival. Because of our expertise in caring for critically ill babies, the overall CDH survival at Children’s Minnesota is 86%. That includes a survival rate over 80% even for babies with severe CDH who require ECMO.
Will my baby require long-term follow up?
Yes, because of all the potential issues associated with CDH, we have developed a comprehensive long term congenital diaphragmatic hernia treatment and follow up plan for our babies with CDH. Your baby’s long term follow up team will include a pediatrician to coordinate your babies overall care, a pulmonary (lung) specialist, a developmental specialist, and any other care giver your baby may require.
Contact us
Need a referral or more information? You or your provider can reach the Midwest Fetal Care Center at 855-693-3825.
