What is fetal anemia?
Fetal anemia is a condition in which a baby’s red blood cell volume falls below normal levels while the baby is developing in the womb. The condition may occur because not enough red blood cells are being produced or because they are being destroyed faster than they can be made. Red blood cells contain hemoglobin, which are molecules that carry oxygen throughout the body. The cells and organs of a developing baby need sufficient amounts of oxygen for nourishment.
Fetal anemia can cause a baby’s heart to beat faster. The heart has to work harder in order to pump more blood and oxygen through the body. In severe cases, the condition can cause the heart to fail. As the heart fails, fluid gathers in the baby’s body around the heart, lungs, and other organs. This abnormal fluid buildup is known as
hydrops fetalis. If untreated, fetal anemia puts the baby’s life at risk.
Who will be on my care team?
At the Midwest Fetal Care Center, a collaboration between Children’s Minnesota and Allina Health, we specialize in individual attention that starts with you having your own personal care coordinator to help you navigate your baby’s treatment process. We use a comprehensive team approach to fetal anemia and any associated conditions. That way, you are assured of getting the best possible information by some of the most experienced physicians in the country. For fetal anemia, your care team will include a maternal-fetal specialist, a pediatric cardiologist, a neonatologist, a nurse specialist care coordinator, a fetal care clinical social worker, and several other technical specialists. This entire team will follow you and your baby closely through the evaluation process, and will be responsible for designing and carrying out your complete care plan
.
Meet the team
What causes fetal anemia?
Fetal anemia most commonly occurs when the mother and baby have incompatible blood types. The most frequent cause is Rh incompatibility—when the mother has Rh-negative blood type and the baby has Rh-positive blood type. The mother’s immune system treats the baby’s Rh-positive red blood cells as “foreign invaders” and sends out antibodies to fight them. The antibodies pass through the placenta and attach to the baby’s red blood cells. The baby’s own immune system then kicks in to fight the invading antibodies. That reaction leads to the destruction of many of the baby’s red blood cells.
Some congenital infections (infections passed from the mother to the baby before birth), such as parvovirus B19 (fifth disease), can also cause fetal anemia. These conditions may temporarily stop the production of the baby’s red blood cells.
Yet another cause of fetal anemia is twin anemia polyeythemia sequence (TAPS), a condition that may develop during pregnancies involving identical twins, who share a placenta. In rare cases, the blood from the shared placenta becomes unevenly distributed between the twins. One twin may receive too little blood, resulting in a low level of red blood cells.
Fetal anemia is also associated with certain genetic and metabolic disorders, such as Down syndrome (Trisomy 21) and Niemann-Pick disease.
How is fetal anemia diagnosed?
The mother’s blood will be tested for the presence of antibodies associated with red blood cell incompatibility that can put the baby at risk of developing anemia. This test is done routinely early in pregnancy and then again at around the 28
th week of pregnancy.
If the blood test shows evidence of antibodies that may lead to fetal anemia, further tests will be done. Among those tests are ones to determine the blood type of the baby. One way of doing this is by testing the blood type of the father of the baby. If a mother’s blood type is Rh negative and the father’s is Rh positive, there is a good chance the baby has Rh positive blood, which puts the baby at risk of developing fetal anemia.
There are other ways of determining the baby’s blood type while the baby is in the womb. Because some of the baby’s DNA (genetic material) is normally in the mother’s bloodstream, for certain blood types the baby’s blood type can be assessed by examining this genetic material in the mother’s blood. Another way of making this assessment is by testing the cells in a sample of amniotic fluid drawn by amniocentesis. This procedure is straightforward and can be done in our clinic. A small needle is placed through the mother’s abdomen and into the amniotic sac surrounding the baby to obtain the fluid sample.
How is fetal anemia managed before birth?
Mothers who test positive for red blood cell antibodies and whose babies are at risk for developing anemia will have regular evaluations to assess how many antibodies are being made. Once a “critical” antibody level is reached in the mother’s blood, high-resolution ultrasound will be used to regularly assess the baby for evidence of anemia.
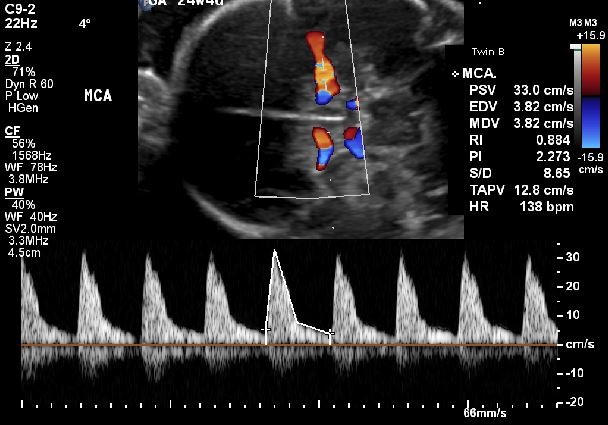
High-resolution fetal ultrasonography is a non-invasive test performed by one of our ultrasound specialists. The test uses reflected sound waves to create images of your baby within the womb. It is very accurate in detecting fetal anemia. It can measure the flow of blood through one of the arteries in your unborn baby’s brain—the middle cerebral artery, or MCA. Blood flow through that artery is faster than normal when fetal anemia is present. High-resolution ultrasound can also identify evidence of fetal hydrops if the anemia is severe enough. (See figure below.)
If the MCA blood flow is found to be elevated, your doctor may recommend fetal blood sampling. This procedure is similar to amniocentesis, but blood is taken from the umbilical cord rather than just fluid from the amniotic sac. Ultrasound will be used so that the doctor can guide the needle through the womb and into a tiny blood vessel in the umbilical cord.
If your baby’s fetal anemia is mild, all that may be required is careful monitoring of the condition during the pregnancy. This may entail periodic high-resolution ultrasound tests to measure the flow of blood through the baby’s MCA.
If the condition is more severe, your baby may need one or several blood transfusions while in the womb. During this procedure, red blood cells are transfused through the vein in the umbilical cord. The transfusions can be done on an outpatient basis, but sometimes the mother stays overnight in the hospital for careful monitoring.
How is fetal anemia treated after birth?
Infants with fetal anemia can be delivered vaginally. Our goal will be to have your baby’s birth occur as near to your due date as possible, usually around the 37th or 38th week of pregnancy. Your baby will be born at The Mother Baby Center at Abbott Northwestern and Children’s Minnesota in Minneapolis or at The Mother Baby Center at United and Children’s Minnesota in St. Paul. Children’s Minnesota is one of only a few centers nationwide with a birth center located within the hospital complex. This means that your baby will be born just a few feet down the hall from our newborn intensive care unit (NICU). Also, many of the physicians you have already met will be present during or immediately after your baby’s birth to help care for your baby right away. Infants with fetal anemia are often born with jaundice. When infants have jaundice, their skin and the whites of their eyes will look yellowish. This condition occurs when the baby’s blood contains an excess amount of bilirubin, a yellow pigment found in blood. Destruction of red blood cells can lead to high levels of bilirubin. Mild cases of jaundice usually require only careful monitoring, as the condition often goes away on its own within two or three weeks. Severe cases may need treatment to bring down the bilirubin levels. That treatment may include phototherapy (exposing the baby’s skin to a special type of light that helps dissolve the excess bilirubin). Infants who undergo multiple transfusions will need to be monitored closely by their doctor during their first month or two. It sometimes takes time for a baby to start making enough of their own red blood cells. Also, some of the mother’s antibodies will persist for a period of time in the baby’s blood, where they will continue to destroy new red blood cells. A blood transfusion (replacing the baby’s blood with blood from a donor to quickly raise the amount of red blood cells) may also be necessary to keep the baby’s blood count at a safe level. In cases of Rh incompatibility, the baby may also be given intravenous immunoglobulin (IVIG) infusions. The immunoglobulin contains antibodies to help keep the baby’s red blood cells from being destroyed. That also keeps the bilirubin in the baby’s blood from rising.
How long will my baby be in the hospital?
Most babies who received treatment in the womb for fetal anemia require no additional time in the hospital after their birth. Some, however, may need to remain in the hospital for a few days for ongoing phototherapy to treat jaundice.
What is my baby’s prognosis?
Babies who receive treatment for fetal anemia have an excellent prognosis.
Will my baby need long-term follow-up care?
Your baby will not need any long-term care for fetal anemia, although such care may be required for babies who have other conditions sometimes associated with fetal anemia, such as Down syndrome or Niemann-Pick disease.
Contact us
Need a referral or more information? You or your provider can reach the Midwest Fetal Care Center at
855-693-3815.
