What is unilateral and bilateral renal agenesis?
Renal agenesis (REE-nall ay-JEN-eh-sis) is a condition in which one or both kidneys fail to form while a baby is developing in the womb. When only one kidney forms, the condition is known as unilateral renal agenesis. When neither kidney forms, it’s known as bilateral renal agenesis. Unilateral renal agenesis occurs in about 1 in 2,000 births. Bilateral renal agenesis is more rare, occurring in about 1 in 4,000 births. Both conditions are about three times more common among boys than among girls.
Kidneys form between the fifth and 12th week of pregnancy, and begin producing urine by the 13th week. A baby’s urine is the major contributor to the amount of protective liquid—amniotic fluid—that surrounds the baby in the womb (Figure 1). In addition to containing important nutrients, hormones, and antibodies, amniotic fluid plays a crucial role in all aspects of the baby’s development, especially lung development.
As long as there is a single healthy kidney with normal amniotic fluid volume, babies born with unilateral renal agenesis generally have no health problems. In about 50 percent of cases, however, the condition is accompanied by additional birth defects. These defects most commonly involve the urinary system, the genitals, the heart, and the central nervous system (the brain and spinal cord).
Babies with bilateral renal agenesis who receive no medical intervention before birth do not usually survive. They are either born stillborn or die shortly after birth, primarily because their lungs have failed to fully develop. A clinical trial involving an experimental therapy for babies diagnosed with bilateral renal agenesis is currently underway. This trial consists of medical interventions that are performed both before and after birth.

Who will be on my care team?
At the Midwest Fetal Care Center, a collaboration between Children’s Minnesota and Allina Health, we specialize in individual attention that starts with you having your own personal care coordinator to help you navigate your baby’s treatment process. We use a comprehensive team approach to renal agenesis and any associated conditions. That way, you are assured of getting the best possible information by some of the most experienced physicians in the country. For renal agenesis, your care team will include an obstetrician or midwife, a maternal-fetal specialist, a pediatric kidney specialist, a neonatologist, a pediatric surgeon, a geneticist, a nurse specialist care coordinator, a fetal care clinical social worker, ultrasonographers, and several other technical specialists. This entire team will follow you and your baby closely through the evaluation process, and will be responsible for designing and carrying out your complete care plan. Meet the team
What causes renal agenesis?
Renal agenesis occurs when two embryonic structures — the ureteric bud and the metanephric blastema — fail to get together to form kidneys during the early weeks of the baby’s development. Scientists aren’t always sure why this failure occurs.
Renal agenesis is usually not inherited, although certain gene mutations have been identified as being associated with the condition. These mutations can be passed on from either parent.
Some research suggests that environmental factors, such as exposures to certain medications or toxins during pregnancy, may play a role in the development of renal agenesis. Studies have also found that women who are obese, who smoke, or who drink alcohol during pregnancy (particularly binge drinking during the second month of pregnancy) may be at increased risk of having a baby with renal agenesis. The mother’s use of illicit drugs, such as cocaine, during pregnancy has also been linked to the condition.
Most cases of renal agenesis, however, are not the result of any behaviors of the mother.
How is renal agenesis diagnosed?
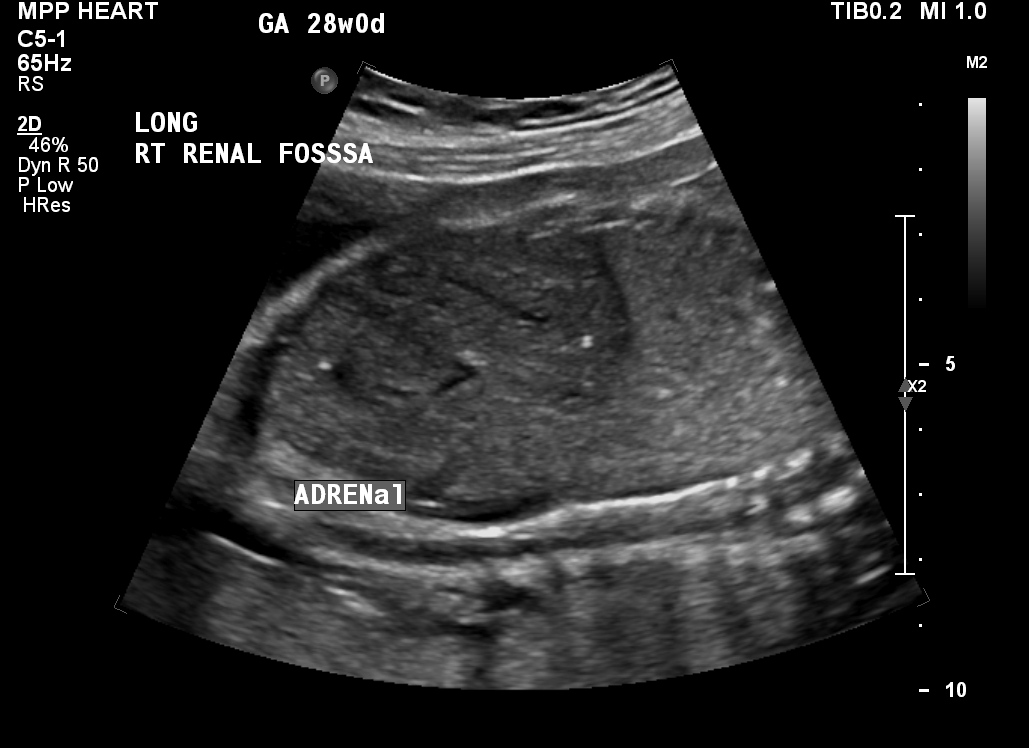
Renal agenesis is usually identified during a routine prenatal ultrasound. The initial telltale sign of the condition is an empty space (renal fossa) where the kidney should be (Figure 2). Also, the adrenal gland — a pyramid-shaped structure usually attached to the top of a kidney — will appear flat on the ultrasound, as if it were “lying down” (Figure 3).
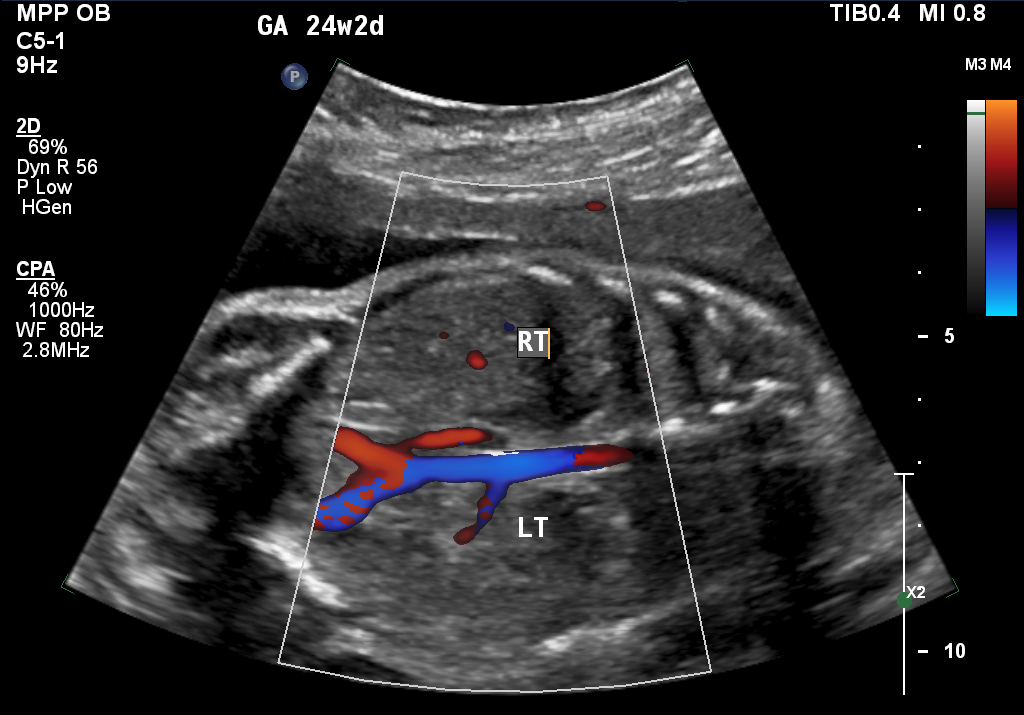
Kidneys can sometimes develop in the wrong place within a baby’s body, a condition known as an ectopic kidney. To rule out that possibility, your doctor will perform an ultrasound scan, which uses sound waves to identify your baby’s anatomic structures. It can also measure the flow of blood through the baby’s blood vessels. Your doctor will look at the ultrasound images to attempt to identify renal (kidney) tissue and renal arteries, which carry blood from the heart to each of the kidneys. The absence of renal tissue, along with the absence of the renal artery on the same side (Figure 4), confirms the diagnosis of renal agenesis.
If no renal tissue is identified and the ultrasound also shows no amniotic fluid in the womb, the diagnosis is likely to be bilateral renal agenesis. The presence of renal tissue with a lack of fluid could be a sign, however, that the membrane around the amniotic fluid — the amniotic sac — has ruptured. Your doctor will either confirm or rule out this possibility by performing a pelvic examination to look for signs of pooled amniotic fluid in the vagina. Other tests may also be done to evaluate for the presence of amniotic fluid, which is usually not found in the vagina.

How is unilateral renal agenesis managed before birth?
If your baby is missing a single kidney, the prenatal care you receive will center on acquiring as much information about the baby’s condition as possible so that we can be prepared during and after delivery to provide optimal care. That includes collecting information on other possible birth defects.
We use several different techniques to gather that information, including high-resolution ultrasonography and fetal echocardiogram. If these tests reveal no birth defects other than the single missing kidney, your baby will not require any special prenatal treatment. An extra ultrasound may be done in the late second or early third trimester of your pregnancy, but otherwise you will receive routine prenatal care.
What is high-resolution fetal ultrasonography?
High-resolution fetal ultrasonography is a non-invasive test performed by one of our ultrasound specialists. The test uses reflected sound waves to create images of your baby within the womb.
What is fetal echocardiogram?
Fetal echocardiography (“echo” for short) is performed at our center by a pediatric cardiologist (a physician who specializes in fetal heart abnormalities). This non- invasive, high-resolution ultrasound procedure looks specifically at how the baby’s heart is structured and functioning while in the womb. This test is important because babies with birth defects are at increased risk of heart abnormalities.
How is bilateral renal agenesis managed before and after birth?
There are no established treatment guidelines, either before or after birth, for babies who are missing both kidneys. Parents of babies with bilateral renal agenesis have the option of not continuing with the pregnancy or, if they wish to continue with the pregnancy, of having their baby receive palliative care after birth.
Some babies with the condition may qualify for an experimental treatment, known as Renal Anhydramnios Fetal Therapy (RAFT). A clinical trial is currently underway to evaluate whether this intervention can improve survival. The trial is currently recruiting patients. Its goal is to preserve the function of the baby’s lungs before birth by making a series of injections of fluid into the amniotic sac to maintain normal fluid volumes. After birth, the baby will likely need to undergo kidney dialysis. A kidney transplant will likely also be needed at some point during the first few years of life.
During the dialysis procedure, a machine will remove waste products and excess fluid from your baby’s blood—the job that kidneys normally do. During the kidney transplant surgery, a surgeon will place a kidney from a donor into your baby’s abdomen. The kidney will then be attached to nearby blood vessels to enable it to start working.
To qualify for a RAFT clinical trial, a baby must have no other serious birth defects, normal genetic testing, and a good chance of surviving the treatment. Your baby’s doctor can counsel you on whether your baby is a candidate for this experimental therapy.
How is renal agenesis managed after birth?
Infants with umilateral renal agenesis can be delivered vaginally. Our goal will be to have your baby’s birth occur as near to your due date as possible.
If there are any concerns of associated birth defects, your baby may be born at The Mother Baby Center at Abbott Northwestern and Children’s Minnesota in Minneapolis or at The Mother Baby Center at United and Children’s Minnesota in St. Paul. Children’s Minnesota is one of only a few centers nationwide with a birth center located within the hospital complex. This means that your baby will be born just a few feet down the hall from our newborn intensive care unit (NICU). Also, many of the physicians you have already met will be present during or immediately after your baby’s birth to help care for your baby right away.
If your baby has bilateral renal agenesis, we will follow the care plan you made for your baby before the birth.
How long will my baby be in the hospital?
Infants with just one kidney and no other birth defects or health problems are likely to be discharged within the normal time frame for newborns. Infants with bilateral renal agenesis who survive to delivery are likely to have a lengthy hospital stay, whether they are receiving RAFT or not.
What is my baby’s prognosis?
The prognosis for babies with unilateral renal agenesis and no other birth defects is excellent. These children can live normal, healthy lives. Special precautions regarding contact sports may need to be made, however, to protect the single kidney.
People born with one kidney are at increased risk of developing high blood pressure and kidney disease during adulthood. Routine screening with a primary care physician can help identify these problems early, however, to ensure timely and effective treatments.
Will my baby require long-term follow up?
Most babies with unilateral renal agenesis do not require long-term follow-up care. Such follow-up may be necessary, however, for babies with the condition who have additional birth defects. These children may also require surgery and hospitalization to help correct these other defects.
Infants with bilateral renal agenesis who survive after receiving RAFT treatment will need long-term medical care and follow-up.
Contact us
Need a referral or more information? You or your provider can reach the Midwest Fetal Care Center at 855-693-3825.
