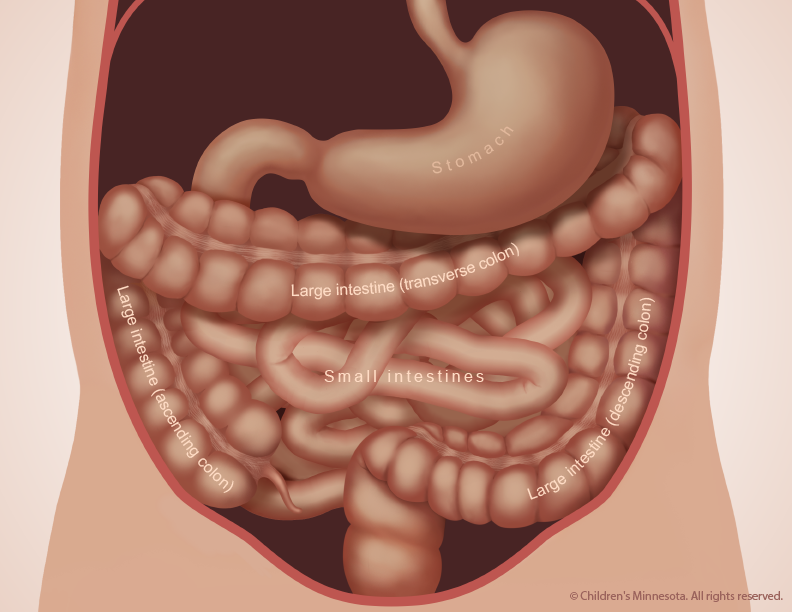
Intestinal atresia (ah-TREE-zha) is a term used to describe a broad spectrum of birth defects that result in a blockage in either the small or large intestine. During normal fetal development, the intestines remain unobstructed, allowing contents from the stomach to flow freely through the baby’s digestive tract (Figure 1). When a blockage (atresia) occurs, however, the intestines lose some or all of their ability to absorb nutrients and to push food and fluids through the baby’s digestive tract.
The severity of intestinal atresia varies, from a defect that causes a partial or small obstruction to the absence of large segments of the affected intestine.
Duodenal (DWAH-de-nal) atresia involves a blockage of the upper part of the small intestine, or duodenum. It results from a different disease process than other types of intestinal atresia and is sometimes associated with additional birth defects. The other types of intestinal atresia are:
Jejunal (je-JOO-nal) atresia, which is a blockage in the jejunum, or middle section of the small intestine;
Ileal (eh-LEE-al) atresia, which is a blockage in the ileum, the final and longest section of the small intestine; and
Colonic (cah-LON-ic) atresia, which is a blockage in the large intestine, or colon.
These conditions are usually isolated anomalies. Babies born with them seldom have other birth defects.
Figure 1 – During normal fetal development, the small and large intestines remains unobstructed
Who will be on my care team?
At Midwest Fetal Care Center, a collaboration between Children’s Minnesota and Allina Health, we specialize in individual attention that starts with you having your own personal care coordinator to help you navigate your baby’s complex treatment process. We use a comprehensive team approach to intestinal atresia. That way, you are assured of getting the best possible information by some of the most experienced physicians in the country. For intestinal atresia, your care team will include a maternal-fetal specialist, a pediatric surgeon, a neonatologist, a nurse specialist care coordinator, a fetal care clinical social worker and several other technical specialists. This entire team will follow you and your baby closely through the evaluation process, and will be responsible for designing and carrying out your complete care plan. Meet the team
What causes intestinal atresia?
Intestinal atresia is a congenital condition, which means it develops before birth. The malformation is thought to be a “vascular accident” that occurs when the blood supply to the unborn baby’s intestines is unexpectedly interrupted. The reason for the reduction in the blood supply is unknown. In most cases it probably occurs sporadically (for no identifiable reason), but some research suggests that certain medications taken during pregnancy may raise the risk. Genetic factors may also play a role.
How is intestinal atresia classified?
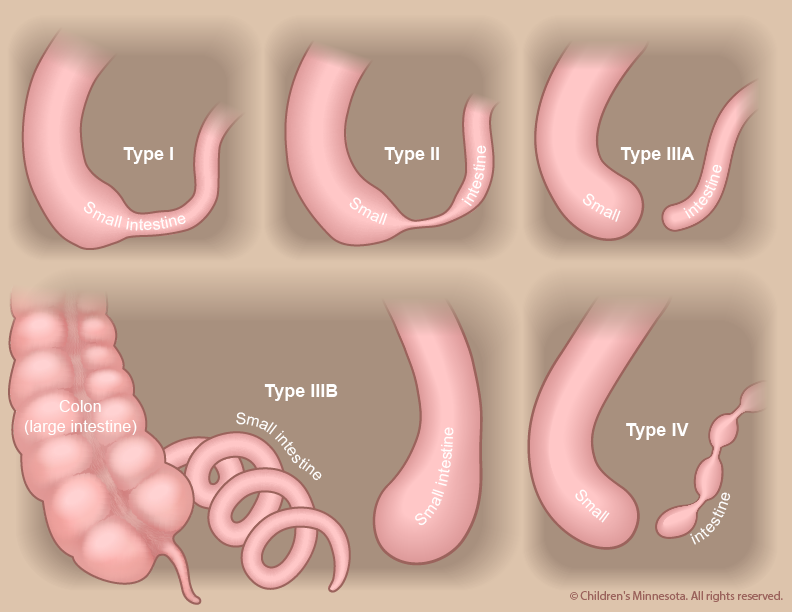
Intestinal atresia is classified according to the cause of the blockage (Figure 2):
Type I atresia: The blockage, which can be partial or complete, is caused by a web-like membrane that forms inside the intestine while the baby is developing in the womb. The baby’s intestine usually grows to normal length.
Type II atresia: The blockage results when one or more segments of the intestine forms a “blind end.” The blind ends are connected by a cord of fibrous tissue, and the baby’s intestine usually grows to normal length.
Type III atresia: In this type of atresia, the segments that end in blind ends are not connected by a fibrous cord. As a result, the blood supply within the intestine is interrupted, and the baby’s intestine usually fails to grow to a normal length. If the end of the intestines below the blockage is not coiled, the blockage is called a type IIIa atresia. Sometimes, however, that end forms a spiral “apple-peel” shape. Such a blockage is known as a type IIIb atresia.
Type IV atresia: The blockage involves many obstructions, giving the intestine a “string-of-sausages” appearance. The blockages may include various combinations of types I, II and III atresia. The baby’s intestine is significantly shorter than normal.
Figure 2 – The type of blockage determines how intestinal atresia is classified.
How is intestinal atresia diagnosed?
A routine ultrasound image taken during pregnancy may show that the baby has a dilated (distended) intestine or, more rarely, that the uterus contains excessive amounts of amniotic fluid (polyhydramnios). Both are potential indicators of intestinal atresia. If these signs are present, a more detailed ultrasound will be done to see if the condition can be confirmed. Most cases of intestinal stenosis and type I atresia are not detected prenatally, but the other classes of intestinal atresia (types II, III and IV) can usually be diagnosed by ultrasound during the third trimester.
How is intestinal atresia managed before birth?
The prenatal management of babies with intestinal atresia starts with acquiring as much information about the condition as early as possible. The information is critical because children with certain classifications of intestinal atresia — types III and IV — have a higher risk of preterm birth. They are also more likely to have shortened intestines. To gather the information, we will use a non-invasive procedure known as high-resolution fetal ultrasonography. In some cases, we may also recommend another non-invasive procedure, fetal magnetic resonance imaging (MRI).
What is high-resolution fetal ultrasonography?
High-resolution fetal ultrasonography is a non-invasive test performed by one of our ultrasound specialists. The test uses reflected sound waves to create images of the baby within the womb. We will use ultrasonography to follow the development of your baby’s intestinal tract — and other internal organs — throughout your pregnancy. We will look for signs of atresia, particularly a dilated intestine. We will also look for signs of polyhydramnios, which may raise the risk of an early delivery.
What is fetal magnetic resonance imaging (MRI)?
Fetal MRI is another non-invasive test. It uses a large magnet, pulses of radio waves and a computer to create detailed images of your baby’s organs and other structures while in the womb. This procedure involves both mom and baby being scanned while partially inside our MRI machine. The test is a bit loud, but it takes only about 30 minutes and is not uncomfortable.
What happens after my evaluation is complete?
After we have gathered all the anatomic and diagnostic information from the tests, our full team will meet with you to discuss the results. Intestinal atresia cannot be definitively treated before a child is born. We will, however, take an active approach to managing the condition during your pregnancy. We will monitor both mother and baby very carefully, looking for any potential complications that might lead to premature delivery. One of those potential complications is polyhydramnios, which can occur when the atresia (blockage) makes it difficult for the baby to swallow. If this happens, we will watch closely for signs of preterm labor and/or symptoms in the mother related to the increased uterine size and pressure.
Occasionally, an amnioreduction is performed. This procedure, which is similar to an amniocentesis, removes some of the excess amniotic fluid and alleviates any symptoms the mother may be experiencing. The procedure is straightforward and can be done in our clinic. It requires numbing the skin on the mother’s belly and placing a small needle through the abdomen and into the amniotic sac to withdraw excess fluid.
How is intestinal atresia treated after birth?
Infants with intestinal atresia can be delivered vaginally. Our goal will be to have your baby’s birth occur as near to your due date as possible. Your baby will be born at The Mother Baby Center at Abbott Northwestern and Children’s Minnesota in Minneapolis or at The Mother Baby Center at United and Children’s Minnesota in St. Paul. Children’s Minnesota is one of only a few centers nationwide with a birth center located within the hospital complex. This means that your baby will be born just a few feet down the hall from our newborn intensive care unit (NICU). Also, many of the physicians you have already met will be present during or immediately after your baby’s birth to help care for your baby right away.
Your baby will need specialized medical care after birth and will therefore be taken to our NICU. Most babies with intestinal atresia are comfortable breathing on their own, but your baby will be unable to nurse or take a bottle and will be fed nutrients intravenously instead. Because your child’s intestine is blocked by the atresia, a thin flexible tube will be inserted into your baby’s stomach through either the nose or mouth. This tube will be used to suck out any air or fluid that collects in the child’s stomach.
Our goal will be to make a definitive diagnosis of intestinal atresia as quickly as possible. That diagnosis can be made with a simple x-ray, done soon after birth.
When will my baby have an operation?
Treatment for intestinal atresia requires an operation to remove the blockage (atresia) and repair the affected part of the intestine. The surgery is not considered an emergency, and is typically done when the baby is two or three days old.
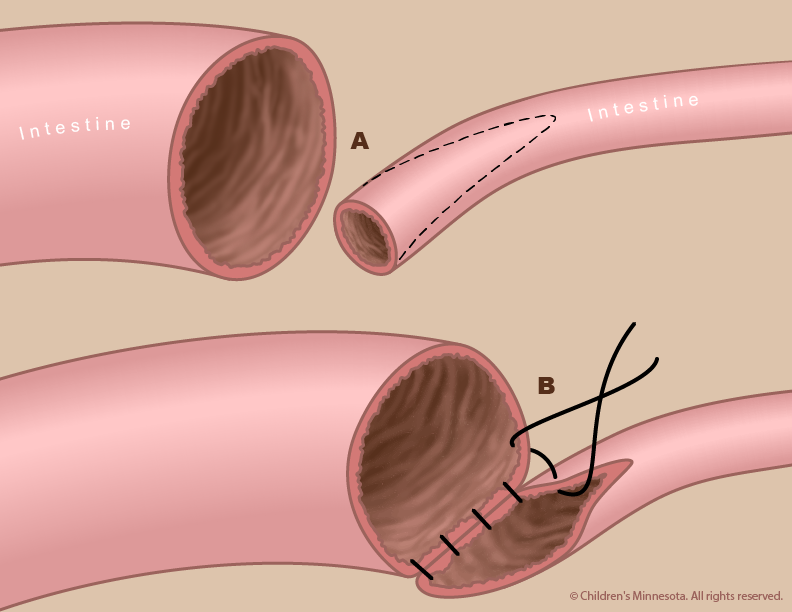
The exact nature of your baby’s surgery will depend on the specific defects in your baby’s intestine. In most cases, the surgeon removes the atresia and then repairs the intestine by sewing the two ends together.
The surgery is done under general anesthesia. Afterward, your baby will be returned to the NICU. For several days, your baby may need a machine (ventilator) to help with breathing.
Figure 3 – After removing the atresia, the surgeon repairs the intestine by sewing the two separated ends together.
How long will my baby be in the hospital?
Babies with intestinal stenosis or type I or II atresia typically remain in the hospital for two or three weeks after their surgery. Babies with type III or IV atresia sometimes have other conditions that may require longer hospitalization. It generally takes one to two weeks after the operation for the baby’s intestines to start working fully, and we usually like to continue to observe the baby in the hospital for a period after that — until the baby is taking food by mouth without difficulty and gaining weight.
What is a central line?
A central line is a special intravenous (IV) catheter that goes deep into your baby’s veins. This catheter allows us to provide your baby with fluids and nutrition while his or her intestines are healing after surgery. The central line will be placed in your baby’s vein by one of our advanced practice neonatal nurse practitioners. This type of central line is known as a percutaneously inserted central catheter (PICC). If your child is unable to have a PICC line, then a surgical central line (Broviac catheter) will be placed in your baby during the operation to repair the intestinal atresia.
What is my baby’s prognosis?
The prognosis for babies with isolated intestinal atresia without associated anomalies is excellent when the condition is diagnosed and treated properly. The prognosis is also good for babies with more severe atresia or with associated anomalies, although they will require more advanced, long-term medical care.
Will by baby require long-term follow-up?
Most babies with isolated intestinal atresia without associated anomalies do not need long-term follow-up. Babies with severe atresia, however, typically require long-term bowel management and intestinal rehabilitation.
Contact us
Need a referral or more information? You or your provider can reach the Midwest Fetal Care Center at 855-693-3825.
Today is Give to Kids Day!
A day for our generous community to join together to ensure that even the tiniest hearts get the strongest possible start.